Comparison of Clinical Effectiveness of Deslorelin Acetate and Osaterone Acetate in Dogs with Benign Prostatic Hyperplasia


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animal Selection
2.2. Indications for Inclusion into Control Group II and Treated Groups III and IV
2.3. BPH Diagnosis
2.4. Drugs and Treatment Schedule
2.5. Study Design
2.6. Statistical Analysis
3. Results
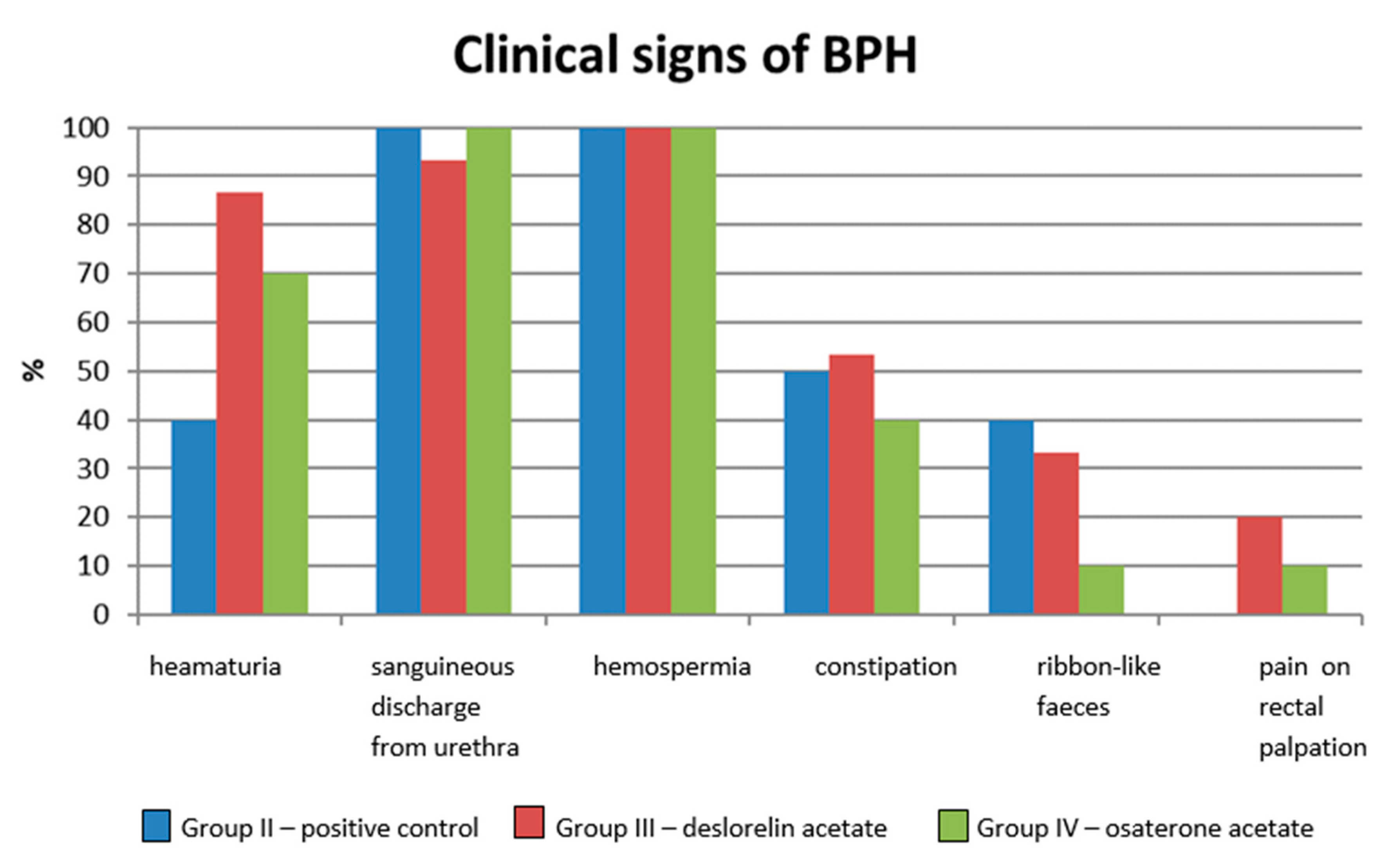
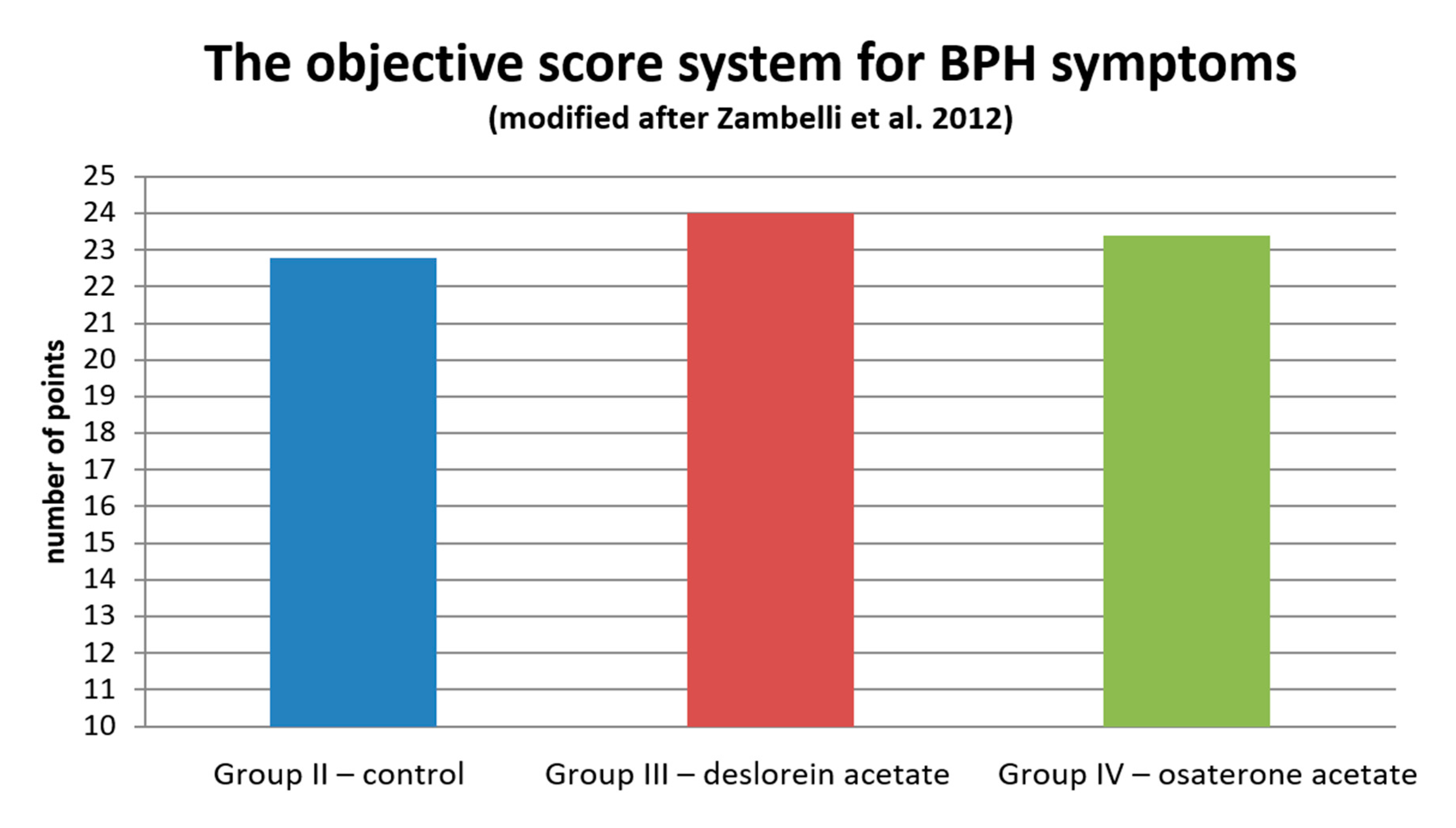
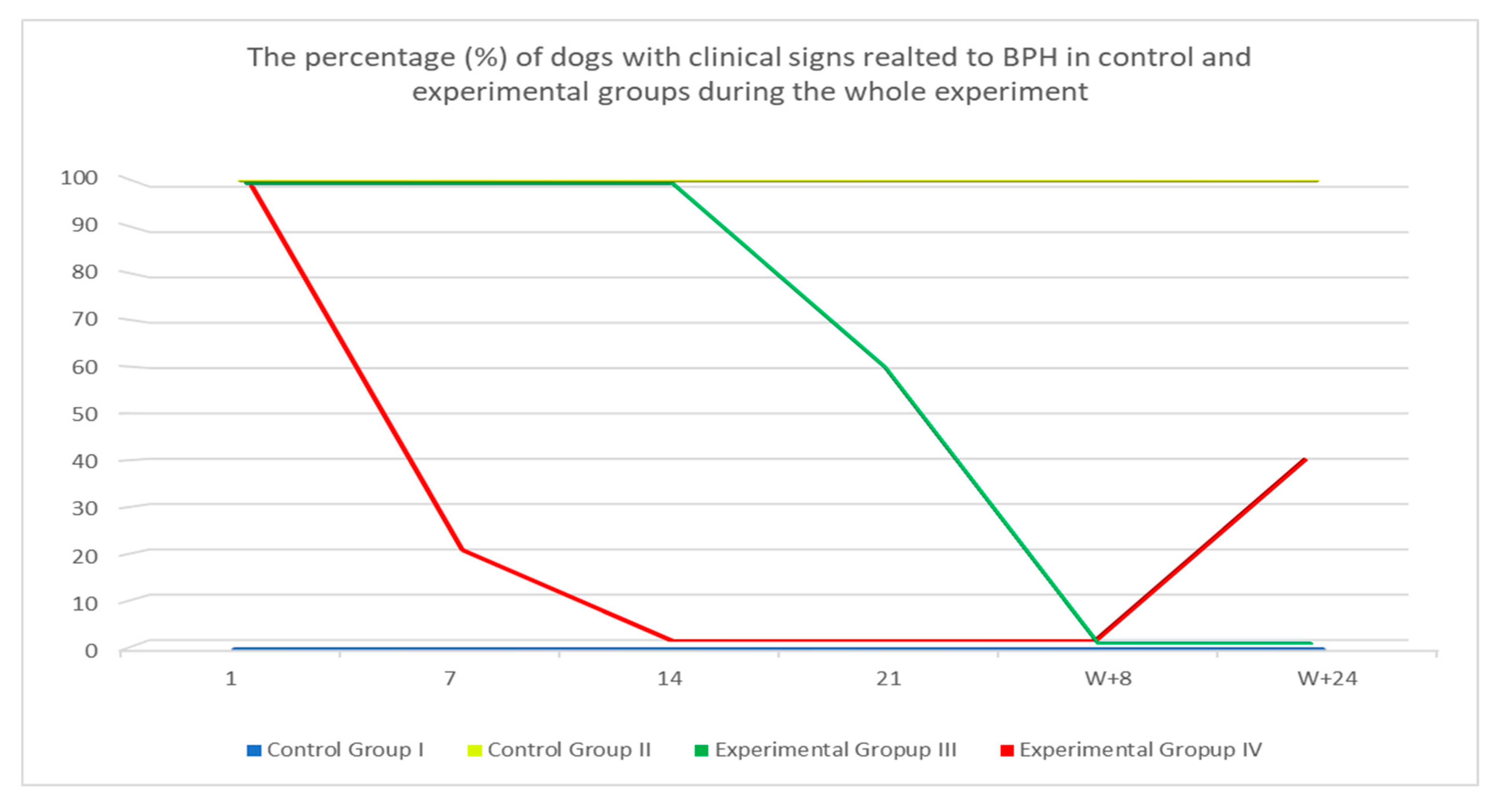
3.1. Clinical Response
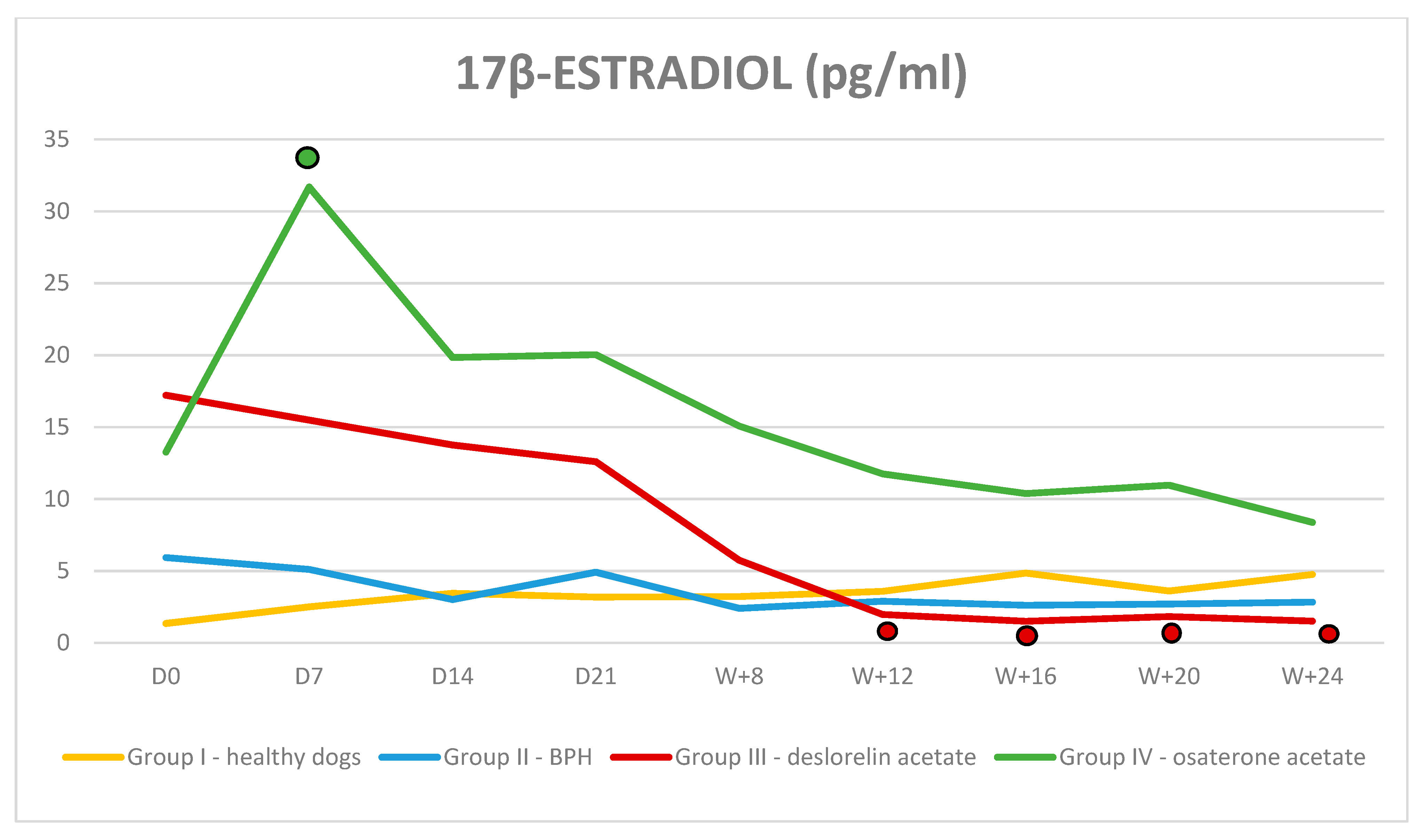
3.2. Hormone Assays and Blood Parameters
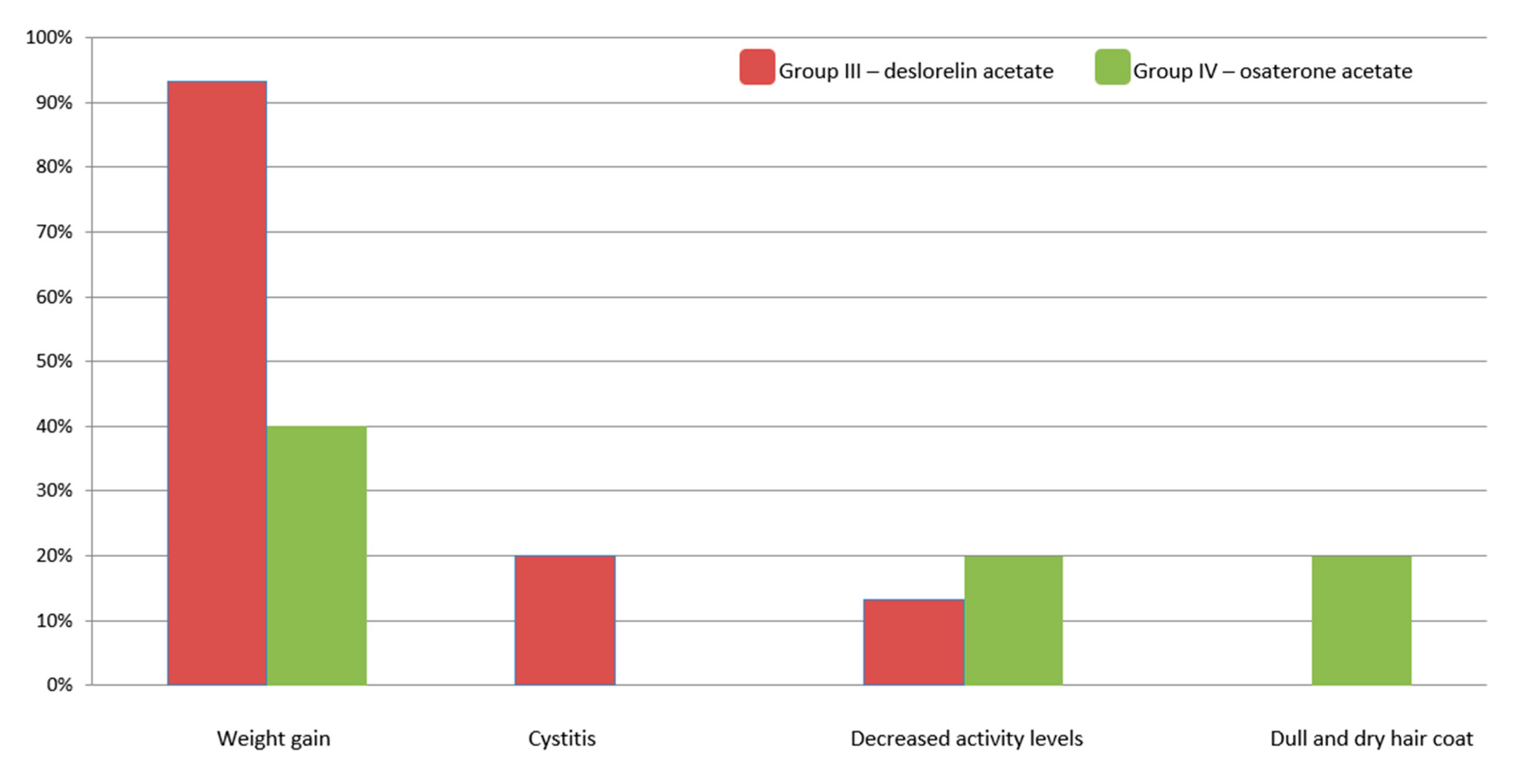
3.3. Treatment-Related Adverse Effect
4. Discussion
4.1. Clinical Efficiency
4.2. Serum Testosterone and 17β-estradiol Levels
4.3. General Blood Results
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Simmons, J.K.; Elshafae, S.M.; Keller, E.T.; McCauley, L.K.; Rosol, T.J. Review of Animal Models of Prostate Cancer Bone Metastasis. Vet. Sci. 2014, 1, 16–39. [Google Scholar] [CrossRef] [Green Version]
- Niżański, W.; Levy, X.; Ochota, M.; Pasikowska, J. Pharmacological Treatment for Common Prostatic Conditions in Dogs–Benign Prostatic Hyperplasia and Prostatitis: An Update. Reprod. Domest. Anim. 2014, 49, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Gobello, C.; Corrada, Y.A. Noninfectious Prostatic Diseases in Dogs. Compend. Contin. Educ. Pract. Vet. 2002, 2, 99–107. [Google Scholar]
- Memon, M.A. Common Causes of Male Dog Infertility. Theriogenology 2007, 68, 322–328. [Google Scholar] [CrossRef]
- Smith, J. Canine Prostatic Disease: A Review of Anatomy, Pathology, Diagnosis and Treatment. Theriogenology 2008, 70, 375–383. [Google Scholar] [CrossRef]
- Lévy, X.; Niżański, W.; von Heimendahl, A.; Mimouni, P. Diagnosis of Common Prostatic Conditions in Dogs: An Update. Reprod Dom Anim. 2014, 49, 50–57. [Google Scholar] [CrossRef]
- Johnston, S.D.; Root-Kustritz, M.V.; Olson, P.N. Disorders of the canine prostate. In Canine and Feline Theriogenology; Johnston, S.D., Root-Kustritz, M.V., Olson, P.N., Eds.; Saunders Co.: Philadelphia, PA, USA, 2001; pp. 337–355. [Google Scholar]
- Lopate, C. The Problem Stud Dog. Vet. Clin. N. Am. Small Anim. Pract. 2012, 42, 469–488. [Google Scholar] [CrossRef]
- Brodbelt, D.C.; Blissitt, K.J.; Hammond, R.A.; Neath, P.J.; Young, L.E.; Pfeiffer, D.U.; Wood, J.L. The risk of death: The confidential enquiry into perioperative small animal fatalities. Vet. Anaesth. Analg. 2008, 35, 365–373. [Google Scholar] [CrossRef]
- Tsutsui, T.; Hori, T.; Shimizu, M.; Orima, H.; Kawakami, E.; Fukuda, S. Regression of Prostatic Hypertrophy by Osaterone Acetate in Dogs. J. Vet. Med. Sci. 2000, 62, 1115–1119. [Google Scholar] [CrossRef] [Green Version]
- Cordaro, M.; Impellizzeri, D.; Siracusa, R.; Gugliandolo, E.; Fusco, R.; Inferrera, A.; Esposito, E.; Di Paola, R.; Cuzzocrea, S. Effects of a co-micronized composite containing palmitoylethanolamide and polydatin in an experimental model of benign prostatic hyperplasia. Toxicol. Appl. Pharmacol. 2017, 15, 231–240. [Google Scholar] [CrossRef]
- Tsutsui, T.; Hori, T.; Shimizu, M.; Tatsuzawa, C.; Kawakami, E. Effect of Osaterone Acetate Administration on Prostatic Regression Rate, Peripheral Blood Hormone Levels and Semen Quality in Dogs with Benign Prostatic Hypertrophy. J. Vet. Med. Sci. 2001, 63, 453–456. [Google Scholar] [CrossRef] [Green Version]
- Albouy, M.; Sanquer, A.; Maynard, L.; Eun, H.N. Efficacies of Osaterone and Delmadinone in Treatment of Benign Prostatic Hyperplasia in Dogs. Vet. Rec. 2008, 163, 179–183. [Google Scholar] [PubMed]
- Socha, P.; Zduńczyk, S.; Tobolski, D.; Janowski, T. The effects of osaterone acetate on clinical signs and prostate volume in dogs with benign prostatic hyperplasia. Pol. J. Vet. Sci. 2018, 21, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Jurczak, A.; Domoslawska, A.; Janowski, T.; Zdunczyk, S. Treatment of Benign Prostatic Hyperplasia (BPH) in dogs using GnRH agonist implant Suprelorin®- preliminary results. In Proceedings of the 7th EVSSAR Congress, Louvain la Neuve, Belgium, 14–15 May 2010; p. 118. [Google Scholar]
- Ponglowhapan, S.; Lohachit, C. Clinical Use of GnRH Agonist Deslorelin in Benign Prostatic Hyperplasia in Dogs. In Proceedings of the 7th EVSSAR Congress, Louvain La Neuve, Belgium, 14–15 May 2010; p. 140. [Google Scholar]
- Polisca, A.; Orlandi, R.; Troisi, A.; Brecchia, G.; Zerani, M.; Boiti, C.; Zelli, R. Clinical Efficacy of the GnRH Agonist (Deslorelin) in Dogs Affected by Benin Prostatic Hyperplasia and Evaluation of Prostatic Blood Flow by Doppler Ultrasound. Rep. Rod. Dom. Anim. 2013, 48, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Kirberger, R.M.; Stander, N. Interventional procedures. In BSAVA Manual of Canine and Feline Ultrasonography; Barr, F., Gaschen, L., Eds.; BSAVA: Gloucester, UK, 2011. [Google Scholar]
- Root Kustritz, M.V. Collection of Tissue and Culture Samples from the Canine Reproductive Tract. Theriogenology 2006, 66, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Zambelli, D.; Cunto, M.; Gentilini, F. Validation of Model to Develop a Symptom Index for Benign Prostatic Hyperplasia in Dogs. Reprod. Dom. Anim. 2012, 47, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Goericke-Pesch, S.; Wilhelm, E.; Ludwig, C.; Desmoulins, P.O.; Driancourt, M.A.; Hoffmann, B. Evaluation of the Clinical Efficacy of Gonazon Implants in the Treatment of Reproductive Pathologies, Behavioral Problems and Suppression of Reproductive Function in the Male Dog. Theriogenology 2010, 73, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Korodi, G.; Igna, V.; Cernescu, H.; Mircu, C.; Frunza, I.; Knop, R. Canine Prostate Pathology. Lucr. Stiintifice Med. Vet. 2008, 41, 187–194. [Google Scholar]
- Murakoshi, M.; Inada, R.; Tagawa, M.; Makino, M.; Suzuki, M.; Mieda, M.; Honma, S.; Takezawa, Y.; Yamanaka, H. Inhibitory Influence of a New Steroid al Antiandrogen, TZP-4238, on Prostatic Hyperplasia in the Beagle Dog. Acta Pathol. Jpn. 1992, 42, 151–157. [Google Scholar]
- Junaidi, A.; Williamson, P.E.; Martin, G.B.; Blackberry, M.A.; Cummins, J.M.; Trigg, T.E. Dose-Response Studies for Pituitary and Testicular Function in Male Dogs Treated with the GnRH Superagonist, Deslorelin. Reprod. Dom. Anim. 2009, 44, 725–734. [Google Scholar] [CrossRef]
- Junaidi, A.; Williamson, P.E.; Cummins, J.M.; Martin, G.B.; Blackberry, M.A.; Trigg, T.E. Use of a New Drug Delivery Formulation of the Gonadotropin-Releasing Hormone Analogue Deslorelin for Reversible Long-Term Contraception in male dogs. Reprod. Fertil. Dev. 2003, 15, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Riesenbeck, A.; Klein, R.; Hoffmann, B. Downregulation, a New and Reversible Approach to Eliminate Testicluar Function in the Dog. Der. Prakt. Tierarzt. 2002, 83, 512–520. [Google Scholar]
- Trigg, T.E.; Wright, P.J.; Armour, A.F.; Williamson, P.E.; Junaidi, A.; Marin, G.B.; Doyle, A.G.; Walsh, J. Use of GnRH Analogue Implant to Produce Reversible, Lpng-Term Suppression of Reproductive Function of Male and Female Domestic Dogs. J. Reprod. Fertil. Suppl. 2001, 57, 255–261. [Google Scholar] [PubMed]
- Trigg, T.E.; Doyle, A.G.; Walsh, J.D.; Swangchan-Uthai, T.A. Review of Advances in the Use of the GnRH Agonist Deslorelin in Control of Reproduction. Theriogenology 2006, 66, 1507–1512. [Google Scholar] [CrossRef]
- Frank, L.A.; Mullins, R.; Rohrbrach, B.W. Variability of Estradiol Concentration in Normal Dogs. Vet. Dermatol. 2010, 21, 490–493. [Google Scholar] [CrossRef]
- Ludwig, C.; Desmoulins, P.O.; Driancourt, M.A.; Goericke-Pesch, S.; Hoffmann, B. Reversible Downregulation of Endocrine and Grminative Testicular Function (Hormonal Castration) in the Dog with the GnRH-Agonist Azagly-Nafarelin as a Removable Implant “Gonazon”; a Preclinical Trial. Theriogenology 2009, 71, 1037–1045. [Google Scholar] [CrossRef]
- Granner, D.K. Hormone Action and Signal Transduction. In Harper’s Illustrated Biochemistry; Murray, R.K., Granner, D.K., Mayes, P.A., Rodwell, V.W., Eds.; The McGraw-Hill Companies: New York, NY, USA, 2003. [Google Scholar]
- Lefebvre, S.L.; Yang, M.; Wang, M.; Elliott, D.A.; Buff, P.R.; Lund, E.M. Effect of age at gonadectomy on the probability of dogs becoming overweight. J. Am. Vet. Med. Assoc. 2013, 243, 236–243. [Google Scholar] [CrossRef]
- Pisani, G.; Millanta, F.; Lorenzi, D.; Vannozzi, I.; Poli, A. Androgen receptor expression in normal, hyperplastic and neoplastic hepatoid glands in the dog. Res. Vet. Sci. 2006, 81, 231–236. [Google Scholar] [CrossRef]




 —indicates p < 0.01 compared to D0 in Group III.
—indicates p < 0.01 compared to D0 in Group III.
—indicates p < 0.01 compared to D0 in Group III.
—indicates p < 0.01 compared to D0 in Group III.
 —indicates p < 0.01 compared to D0.
—indicates p < 0.01 compared to D0.
—indicates p < 0.01 compared to D0.
—indicates p < 0.01 compared to D0.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Breed and Number of Dogs Investigated | Group I | Group II | Group III | Group IV |
|---|---|---|---|---|
| Airedale Terrier | 1 | |||
| Alaskan Malamute | 1 | |||
| American Staffordshire Terrier | 1 | 2 | ||
| Australian Cattle Dog | 1 | 2 | ||
| Beagle | 1 | 1 | ||
| Bedlington Terrier | 1 | |||
| Bernese Mountain Dog | 1 | |||
| Boxer | 2 | |||
| Briard | 1 | |||
| Dachshund | 1 | |||
| German Shepherd | 1 | |||
| German Shorthaired Pointer | 1 | |||
| Irish Setter | 1 | 1 | 1 | |
| Labrador Retriever | 1 | |||
| Leonberger | 1 | 1 | ||
| Miniature Schnauzer | 1 | 1 | ||
| Pointer | 1 | |||
| Polish Hound | 2 | |||
| Shetland Sheepdog | 1 | |||
| Welsh Corgi Cardigan | 2 | |||
| Yorkshire terrier | 2 | 1 | ||
| Cross Breed | 2 | 4 | 4 | |
| Total | 10 | 10 | 15 | 10 |
| Anorexia | Weight Loss | Defecation | Dysuria | Urinary Incontinence | Urinary Leakage | Hematuria | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Amount | Frequency | Duration | Amount | Frequency | Duration | |||||
| 1: absent | 1: absent | 1: normal | 1: normal | 1: absent | 1: absent | 1: absent | 1: absent | 1: absent | 1: absent | 1: absent |
| 2: for 1 day | 2: mild | 2: regular with tenesmus | 2: flow weaker or interrupted very | 2: present | 2: few drops | 2: once in a year | 2: one week | 2: few drops | 2: once in a year | 2: one week |
| 3: 1 to 7 days | 3: moderate | 3: regular with tenesmus | 2: flow weaker or interrupted very | 3: urine | 3: 2–3 times per year | 3: two week | 3: pinkish drops | 3: 2–3 times | 3: two week | |
| 4: > 7 days | 4: severe | 4: absent for last a few days | 4: urinary retention | 4: copious | 4: > 3 times per year | 4: > 15 days | 4: red urine | 4: >3 times per year | 4: > 15 days | |
| Parameter | RBC (T/L) | HGB (mmol/L) | HCT (L/L) | MCV (f/L) | MCH (f/ML) | |||||||||||||||
| Group | I | II | III | IV | I | II | III | IV | I | II | III | IV | I | II | III | IV | I | II | III | IV |
| D0 | 6.67 ± 0.83 | 7.3 ± 0.5 | 7.61 ± 1.34 | 7.16 ± 0.92 | 9.68 ± 1.13 | 11.19 ± 2.19 | 9.99 ± 0.92 | 9.87 ± 1.34 | 0.49 ± 0.07 | 0.53 ± 0.03 | 0.51 ± 0.05 | 0.51 ± 0.07 | 73.1 ± 3.14 | 71.5 ± 2.84 | 73.01 ± 3.35 | 71.2 ± 4.02 | 1.45 ± 0.07 | 1.41 ± 0.05 | 1.45 ± 0.08 | 1.38 ± 0.09 |
| T + 8 | 6.5 ± 0.48 | 7.13 ± 0.42 | 6.91 ± 0.54 | 6.13 ± 1.24 | 9.51 ± 0.81 | 10.03 ± 0.44 | 9.91 ± 0.81 | 8.5 ± 1.68 | 0.47 ± 0.05 | 0.51 ± 0.02 | 0.5 ± 0.04 | 0.43 & ± 0.09 | 72.67 ± 3.46 | 71.8 ± 1.55 | 72.87 ± 3.29 | 70 ± 4.85 | 1.46 ± 0.08 | 1.41 ± 0.04 | 1.42 ± 0.07 | 1.39 ± 0.14 |
| T + 24 | 6.57 ± 0.5 | 6.52 * ± 0.79 | 7.1 ± 0.56 | 7.16 ± 0.92 | 9.6 ± 1.01 | 9.4 * ± 1.14 | 10.66 ± 1.62 | 9.87 ± 1.34 | 0.48 ± 0.05 | 0.47 * ± 0.06 | 0.51 ± 0.05 | 0.51 ± 0.07 | 72.56 ± 3.78 | 71.6 ± 1.51 | 72.33 ± 3.27 | 71.2 ± 4.02 | 1.46 ± 0.06 | 1.44 ± 0.03 | 1.44 ± 0.08 | 1.38 ± 0.09 |
| Parameter | RBC (T/L) | HGB (mmol/L) | HCT (L/L) | MCV (f/L) | MCH (f/ML) | |||||||||||||||
| Group | I | II | III | IV | I | II | III | IV | I | II | III | IV | I | II | III | IV | I | II | III | IV |
| D0 | 6.67 ± 0.83 | 7.3 ± 0.5 | 7.61 ± 1.34 | 7.16 ± 0.92 | 9.68 ± 1.13 | 11.19 ± 2.19 | 9.99 ± 0.92 | 9.87 ± 1.34 | 0.49 ± 0.07 | 0.53 ± 0.03 | 0.51 ± 0.05 | 0.51 ± 0.07 | 73.1 ± 3.14 | 71.5 ± 2.84 | 73.01 ± 3.35 | 71.2 ± 4.02 | 1.45 ± 0.07 | 1.41 ± 0.05 | 1.45 ± 0.08 | 1.38 ± 0.09 |
| T + 8 | 6.5 ± 0.48 | 7.13 ± 0.42 | 6.91 ± 0.54 | 6.13 ± 1.24 | 9.51 ± 0.81 | 10.03 ± 0.44 | 9.91 ± 0.81 | 8.5 ± 1.68 | 0.47 ± 0.05 | 0.51 ± 0.02 | 0.5 ± 0.04 | 0.43 & ± 0.09 | 72.67 ± 3.46 | 71.8 ± 1.55 | 72.87 ± 3.29 | 70 ± 4.85 | 1.46 ± 0.08 | 1.41 ± 0.04 | 1.42 ± 0.07 | 1.39 ± 0.14 |
| T + 24 | 6.57 ± 0.5 | 6.52 * ± 0..79 | 7.1 ± 0.56 | 7.16 ± 0.92 | 9.6 ± 1.01 | 9.4 * ± 1.14 | 10.66 ± 1.62 | 9.87 ± 1.34 | 0.48 ± 0.05 | 0.47 * ± 0.06 | 0.51 ± 0.05 | 0.51 ± 0.07 | 72.56 ± 3.78 | 71.6 ± 1.51 | 72.33 ± 3.27 | 71.2 ± 4.02 | 1.46 ± 0.06 | 1.44 ± 0.03 | 1.44 ± 0.08 | 1.38 ± 0.09 |
| Parameter | PLT (G/L) | WBC (G/L) | LYM (%) | MON (%) | GRA (%) | |||||||||||||||
| Group | I | II | III | IV | I | II | III | IV | I | II | III | IV | I | II | III | IV | I | II | III | IV |
| D0 | 286.3 ± 98.1 | 306.7 ± 100.88 | 261.13 ± 58.51 | 278.1 ± 125.71 | 8.89 ± 2.17 | 8.57 ± 1.89 | 7.61 ± 1.34 | 8.53 ± 2.4 | 14.23 ± 4.18 | 16.57 ± 3.37 | 14.31 ± 3.97 | 12.14 ± 2.91 | 4.82 ± 1.45 | 4.53 ± 0.84 | 5.28 ± 1.77 | 5.52 ± 2.3 | 80.95 ± 5.28 | 78.9 ± 3.81 | 80.41 ± 4.72 | 82.34 ± 4.9 |
| T + 8 | 292 ± 112.71 | 281.3 ± 97.18 | 262.27 ± 61.99 | 313.5 ± 148.6 | 9.37 ± 2.57 | 9.03 ± 2.9 | 7.01 ± 1.09 | 6.92 ± 2.61 | 13.09 ± 3.51 | 18.49 & ± 2.49 | 15.13 ± 3.75 | 15.47 ± 3.02 | 4.3 ± 1.9 | 5.11 ± 1.21 | 5.13 ± 1.37 | 5.88 ± 1.87 | 82.61 ± 4.34 | 76.4 ± 3.32 | 79.74 ± 4.89 | 78.65 ± 3.91 |
| T + 24 | 307.44 ± 88.53 | 269.1 ± 76.68 | 264.33 ± 82.14 | 278.1 ± 125.71 | 9.06 ± 2.1 | 9.8 ± 2.98 | 7.67 ± 1.41 | 8.53 ± 2.39 | 14.78 ± 5.11 | 16.12 ± 2.97 | 15.19 ± 4.21 | 12.14 ± 2.91 | 4.87 ± 1.53 | 4.62 ± 1.05 | 4.95 ± 1.23 | 5.52 ± 2.3 | 80.36 ± 6.08 | 79.26 ± 3.64 | 79.87 ± 5.25 | 82.34 ± 4.9 |
| Parameter | ALT (U/l) | AST (U/l) | ALP (U/l) | CREA (mg/dl) | UREA (mg/dl) | |||||||||||||||
| Group | I | II | III | IV | I | II | III | IV | I | II | III | IV | I | II | III | IV | I | II | III | IV |
| D0 | 53.94 ± 21.85 | 41.21 ± 19.08 | 57.94 ± 17.05 | 55.8 ± 40.17 | 31.15 ± 8.31 | 24.75 ± 8.21 | 29.89 ± 4.15 | 30.16 ± 7.65 | 23.42 ± 13.98 | 20.74 ± 3.77 | 36.42 ± 30.96 | 29.18 ± 15.89 | 0.93 ± 0.16 | 0.96 ± 0.27 | 0.91 ± 0.22 | 0.94 ± 0.19 | 33.71 ± 12.56 | 41.69 ± 10.01 | 36.65 ± 8.05 | 41.69 ± 27.55 |
| T + 8 | 55.32 ± 14.37 | 49.78 ± 33.44 | 58.59 ± 40.7 | 51.62 ± 25.27 | 27.46 ± 7.06 | 26.85 ± 5.64 | 31.81 ± 8.65 | 26.73 ± 3.2 | 19 ± 0 | 22.34 ± 8.92 | 28.75 ± 23.59 | 52.27 ± 93.17 | 0.89 ± 0.19 | 0.89 ± 0.21 | 1.01 ± 0.28 | 1.01 ± 0.34 | 39.78 ± 10.62 | 42.36 ± 21.48 | 45.22 * ± 10.43 | 43.61 ± 27.49 |
| T + 24 | 55.79 ± 20.66 | 49.31 ± 12.98 | 58.65 ± 47.33 | 43.22 ± 17.18 | 27.42 ± 5.63 | 31.29 ± 8.66 | 33.13 ± 9.77 | 29.63 ± 6 | 19 ± 0 | 28.13 ± 21.9 | 28.63 ± 22.99 | 42.62 ± 41.01 | 37.9 ± 0.17 | 0.94 ± 0.24 | 0.98 ± 0.3 | 1.03 ± 0.45 | 37.9 ± 12.65 | 49.7 ± 20.61 | 41.91 ± 11.59 | 39.65 ± 24.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niżański, W.; Ochota, M.; Fontaine, C.; Pasikowska, J. Comparison of Clinical Effectiveness of Deslorelin Acetate and Osaterone Acetate in Dogs with Benign Prostatic Hyperplasia . Animals 2020, 10, 1936. https://doi.org/10.3390/ani10101936
Niżański W, Ochota M, Fontaine C, Pasikowska J. Comparison of Clinical Effectiveness of Deslorelin Acetate and Osaterone Acetate in Dogs with Benign Prostatic Hyperplasia . Animals. 2020; 10(10):1936. https://doi.org/10.3390/ani10101936
Chicago/Turabian StyleNiżański, Wojciech, Małgorzata Ochota, Christelle Fontaine, and Joanna Pasikowska. 2020. "Comparison of Clinical Effectiveness of Deslorelin Acetate and Osaterone Acetate in Dogs with Benign Prostatic Hyperplasia " Animals 10, no. 10: 1936. https://doi.org/10.3390/ani10101936